Bone Augmentation Upper and Lower Jaw
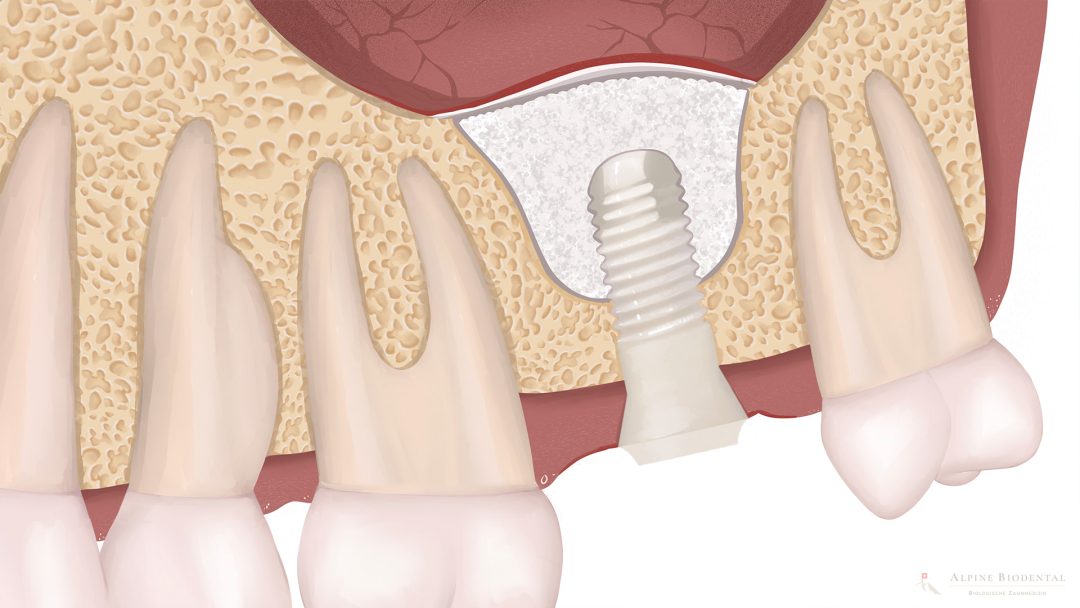
If bone height and width are insufficient for a dental implant, bone augmentation can be performed in the upper and lower jaw.
From a health perspective, it is advantageous to use autogenous bone. Autogenous bone can be in the form of bone chips or a block of bone.
Bone chips are preferably collected in a sterile bone collector (e.g., Safescraper) and introduced into the bone defect without contamination.
A bone block is gently and precisely harvested using piezosurgery and then placed in the correct location. It heals with the existing bone, improving bone availability both horizontally and vertically.
The use of bone substitutes should be avoided if possible, as foreign material can lead to local inflammation. However, if there is no alternative, the material should be chosen to optimize biology and promote complete bone transformation.
A special form of bone augmentation in the upper jaw is the so-called sinus lift.
Related topics
Sinus Lift
Sinus lift is a special type of bone augmentation that can be performed in the maxillary sinus area to provide more bone.

Dr. med. dent. Josephine Phillips
Bone augmentation may be necessary before an implantation. The correct material and a careful approach are crucial.

Further information
The following relevant information is listed to provide you with more insight into the topic.